Corneal Lacerations
Corneal lacerations are usually considered an emergency, with prompt referral important for optimal outcomes. Corneal lacerations frequently result from cat-scratch injuries in dogs and cats. Puppies are commonly injured as they are curious and have not yet learned to read hostile signals.
Signs of corneal laceration include:
- red eye
- cloudy eye
- discharge (serous, mucopurulent)
- iris prolapse (black lesion on the cornea)
- ocular pain (blepharospasm, third eyelid elevation)
Corneal lacerations can be linear, or jagged and can be partial thickness or full thickness. Four prognostic indicators should be considered with corneal lacerations:
- The depth of the laceration
- Whether there is intraocular involvement including iris, lens, vitreous and retina
- Any extension of the laceration beyond the limbus into the sclera
- How long the laceration has been present before treatment commenced
In general, superficial corneal injuries carry a better prognosis. Deeper penetrations can be associated with globe perforation and intraocular contamination. With corneal perforation there is an initial escape of aqueous humour with the breach then typically sealing with fibrin, blood or iris. Damage to any intraocular structures needs to be assessed. Larger lens capsule perforation leads to intraocular exposure to lens protein which can result in severe phacoclastic uveitis, often unresponsive to medical treatment. Smaller lens capsule tears may simply result in focal cataract at the site, but later this can affect the entire lens. Other common associated intraocular injuries include iris damage, prolapse and haemorrhage (hyphaema) and intraocular infection (endophthalmitis).
Treatment of corneal lacerations depends on severity, with some mild cases requiring only medical management:
- topical antibiotics to prevent corneal infection
- topical atropine to prevent synechiae (iris adhesions)
- systemic broad-spectrum antibiotics to prevent intraocular infection
- systemic NSAIDs to control secondary uveitis
Surgery is recommended in cases that are full thickness and leaking aqueous and/or more than 3mm in length and/or have any iris prolapse. This usually involves wound edge debridement and suturing with 8-0 or 9-0 absorbable suture, performed with an operating microscope. Occasionally highly mobile or necrotic superficial flaps of superficial cornea may be better trimmed than sutured.
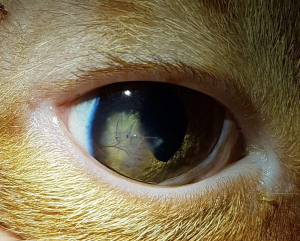
Mr Kittens (picture below pre-surgery, 2 weeks post-surgery and around 3 months post-surgery) is a recent patient that presented to VOR with a triangular full thickness corneal laceration following a suspected cat-scratch injury. Corneal repair with 9-0 PGA suture material resulted in an excellent functional and cosmetic outcome.